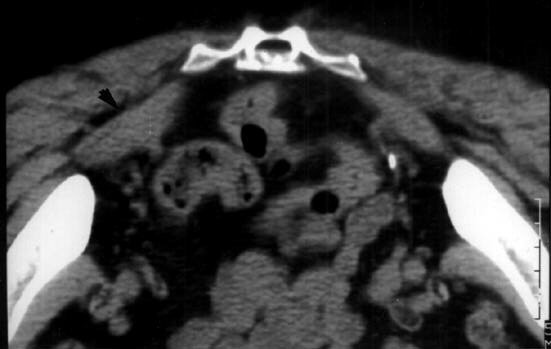
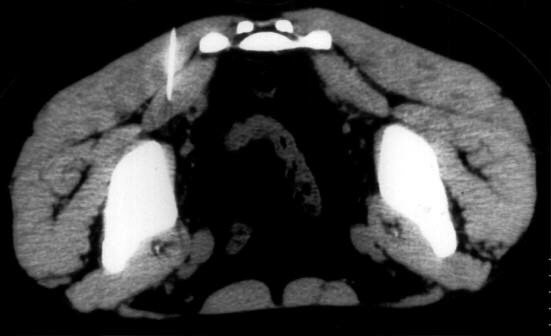
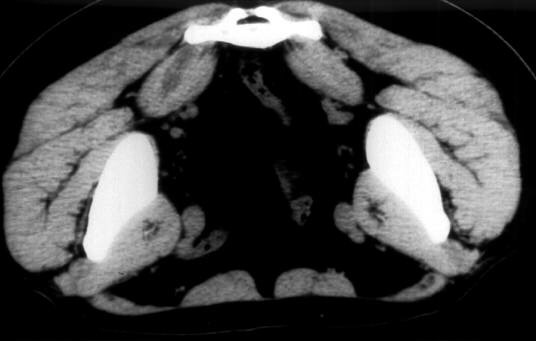
Guided CT treatment with botulinic toxin ( Botox ) in patients suffering from Pyriform Muscle Syndrome.
E.Fanucci,V.Varrucciu, L.Bortolotti,C.Iani*,G. Bernardi*, G.Simonetti
Guided CT treatment with botulinic toxin ( Botox ) in patients suffering from Pyriform Muscle Syndrome.
E.Fanucci,V.Varrucciu, L.Bortolotti,C.Iani*,G. Bernardi*, G.Simonetti