Techniques and interpretation.
E. Squillaci MD, M. Pocek MD,S. Fosi MD, P. Gamba MD, M.G. Ciolfi MD, F. Maspes MD, M.L.Grandinetti MD, G. Simonetti MD
![]()
INTRODUCTION
Spiral CT angiography (CTA) is the latest in a series of technical innovations in vascular imaging which allows for spectacular three-dimensional reconstructions of the blood vessels and organs. Most of the work evaluating the utilityof CTA has been performed in the abdomen, mainly in the aorta and splancnicvessels. With this exibit we demonstrate the technique and the possibilitiesof CTA in the portal venous system.
TECHNIQUE
CM Injection
-Power injector
-16 -18 G needle antecubital vein
-Non ionic e.v. cm
-Oral cm: water
Portal thrombosis Portal hypertention
| Amount | 3 ml/s 150ml | 2 ml/s 180ml |
| Delay | 60 s | 80s |
| Concentration | 370 mgI/ml | 300 mgI/ml |
Acquisition parameters (Philips TOMOSCAN SR 7000)
| -Kvp=120 -mA=250-300 -Matrix=512 X 512 -Interpolation=180° -Rec Index=2mm |
-Slice thickness=3-5mm -Table Feed=5mm/s -Acquisition time=30s -Coverage=15cm -Pitch=1-1.6 |
Reconstruction Techniques
Workstation: Easy Vision CT/MR R2
2D (MPR, CPR) 3D(MIP, SSD)



A B C
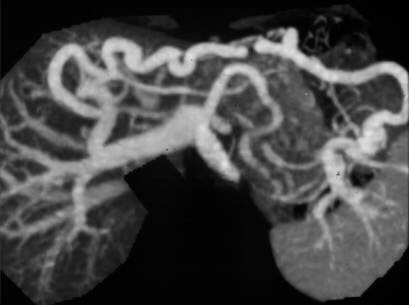
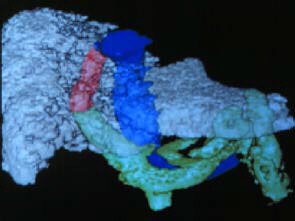
NORMAL ANATOMY OF THE PORTAL VENOUS SYSTEM
A: CPR, B: MIP, C-D: SSD, after subtraction of the liverparenchyma.
CTA FINDINGS
Spleno-portal axis
- Stenosis
- Partial thrombosis
- Complete thrombosis

A B
PORTAL VEIN THROMBOSIS
A: CPR reconstruction of partial thrombosis at the confluence between
splenic and portal vein.
Residual flow is well demonstrated.
B: MIP recontruction of partial thrombosis of the main portal vein.
Collaterals
- Gastro-esophageal
- Spleno-renal
- Porto-hepatic
- Paraumbilical



A B C
COLLATERALS
A: Spleno-renal shunt (MPR).
B-C: Patency of the paraumbilical vein (SSD).
TIPS follow-up
- Patency

A B C
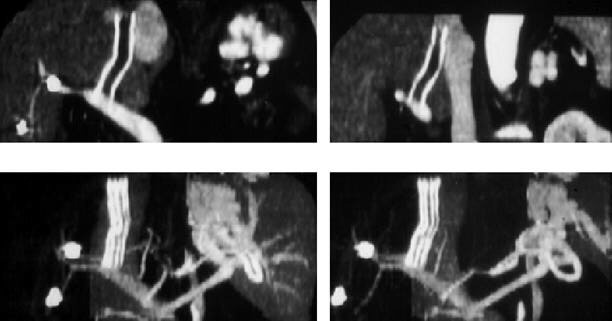
FOLLOW-UP AFTER TIPS
A: CPR allow to follow the stent and to evaluate the relationshipbetween
hepatic and portal vein. Flow inside the stent is well demonstrated.
B: SSD demonstrate only stentposition.
C: Stent thrombosis. MPR (top) demonstrate the absence of flow andthethrombus,
MIP (bottom) the presence of gastric curve collaterals.
Pre-operatory evaluation
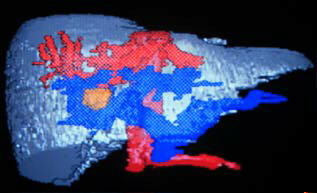
SMALL HEPATIC TUMOR IN A CIRRHOTIC LIVER
SSD images demonstrate the relationship of the tumor with the portal
system
LIMITATIONS
MPR - No significant limitations
CPR - Overlapping of non opacified structures
MIP - Slow venous flow
SSD - Thrombosis
Comparison 2D/3D technique
MPR - CPR MIP SSD
| THROMBOSIS | 2 | 1 | 0 |
| COLLATERALS | 0 | 2 | 1 |
| TIPS | 2 | 1 | 0 |
0 = POOR
1 = GOOD
2 = EXCELLENT
CTA versus MRA
CTA
- Not sensible to turbolent flow
- Visualization of vessels and parenchyma
MRA
- No iodinated cm
- Directional informations
CTA versus color US
CTA
- Large, obese Patients
- Ascites
- Large collaterals
Color US
- Easy and fast
- Quantitative and directional analysis
CONCLUSIONS
Good imaging quality was obtained in all Patients.
Technique of choice for evaluation of PV thrombosis.
Good evaluation of collaterals.
Clinical indications when doppler-US is not conductive, and in casesof very
slow flow.